The pain started about two weeks ago. The outside of my left knee had a very acute jarring sensation every time I started trying to run. The pain increased with hills and speed, but was always there, and after runs I just kind of hobbled around. I started skipping runs to rest the knee, but every time I tried running, the pain came back pretty quickly. After seeing my general practitioner last week, he referred me to a sports rehab physical therapist.
After diagnosing me, Cynthia grabbed a nice big picture book and flipped to a page with the following picture:

My site of pain is just below the little blue circle. Cynthia suspected when I got near the end of my long runs and my form began faltering due to a relatively weak core my IT band just began receiving too much stress (in the reprocessed thoughts of this astronomer) and fought back.
We got out the foam roller, where I did the process below and deeply understood the sentiment in the picture:


I thought we were doing great. I would work out my IT band with a foam roller and walk around like a monster. No problem! Then, Cynthia said, "You're not going to like what I'm going to say next," and I thought, "Sure, whatever!"
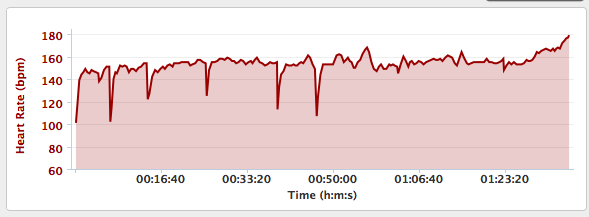
But alas, she proceeded to explain my running was now limited to 20-30 minute repeat sessions of walking for 4 minutes and then running at LSD pace or slower for 1 minute. She's right. I didn't like that. But the bright side is she expects me to be able to return to my full running program in 2-3 weeks.
The obvious downside to this is I most likely will not be running the Madison Marathon. This isn't too surprising. I haven't had a long run in 2 weeks because of this IT band issue. I may try doing the half depending on how strong I'm feeling. We'll just have to wait and see...