
I’ve been training with heart rate monitors (HRMs) for about 3 or 4 years now. The idea is that either by checking your pulse or using a chest strap that detects your beating heart, your heart rate can be measured and transmitted to some device (usually just a watch) that gives you continual updates. I first started to think they might be something useful after riding those stationary bikes at the college gym that had a HRM integrated into the system. But I also hated riding a stationary bike. So, while I was racing and training for my bike ride across America, I opted to buy the cheapest HRM I could find and started using it for all my workouts.

There are a lot of ways that you’re supposed to use the information you gain from a HRM. They’re all related to this idea of a max heart rate and a bunch of other info determined from equations that are not entirely accurate. As such, I almost completely ignore them. So, then why in the world do I use a HRM?
It lets me know how many matches I have to burn.
In cycling, there’s always talk about how all these guys are attacking each other back and forth as they ride up a mountain pass. Each time a rider attacks, the other riders have to quickly accelerate to stay with the guy, or their races are over. And with each of those accelerations, there’s a good chance they’re exerting themselves more than they’d like. The measure of “more than they like” is really what is referred to as a lactate threshold. Once you start crossing that threshold in an endurance race, it’s downhill because lactic acid streams into your blood, making everything hurt just a bit more. And so they’ve burned a match. Eventually, their body has produced so much lactic acid that they’ve burnt through all their matches, and they can no longer keep up with the race’s pace.
Over the years I’ve been able to ascertain a rough region of my heart rate that corresponds to my lactate threshold just by measuring my exertion, pain, and heart rate (I know it’s not the proper way to determine lactate threshold). And so as I run, I can keep an eye on my exertion and how many matches I have to burn via a HRM. It ultimately means I have a better idea what’s going on with my body. And that knowledge helps me dole out my exertions a bit more carefully, so I don’t get burnt out halfway through a run. Additionally, I know that if my heart rate is lower for a given pace and distance than it was a week ago, I now have a tangible artifact showing an increase in strength. This makes my Garmin Forerunner 110 a great device for me. I can monitor my heart rate while knowing what my running pace is and search for correlation.

If you’re interested in training with a HRM the way I do, my (proceed at your own risk) advice is to grab a relatively cheap HRM (usually no more than $50-60). Then over a series of workouts begin watching your heart rate to see how it goes with an exertion. A great way to do this is with interval training, where you briefly (no more than 2-3 minutes) go all out and watch your heart rate to see you at what point you begin physically breaking down. Back off for a few minutes and repeat the heavy effort. With time and consistency, you’ll be able to paint a picture of your body’s limits and can begin stretching them to improve your fitness. It’s kind of a fun thing.
Additionally, after painting this picture, you can then begin using the HRM to understand how much effort you are/should be putting into a given workout. For example, on my LSD runs, I know around what levels I should be keeping my heart rate at and can keep myself in that region.
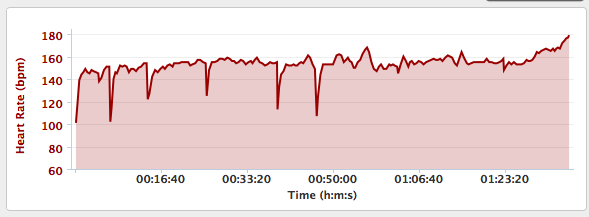
If you’re curious, you can check out the info from my most recent runs with the toolbar on the right. The links open up a page to my Garmin Connect account where you can see my heart rate data coupled with pace, distance, and elevation information. Notice how elevation often correlates pretty closely to heart rate.
Aside: I think it is really easy to get “teched out” with regard to using too many data devices during exercise. I think it’s important for you to understand exactly what you’re looking to get out of using a HRM or GPS watch or whatever else device you have. For me, I settle for the simpler devices because they fit with what I want in my training. For you, that may mean a more elaborate device or, perhaps, no devices. It’s all up to you.
Aside: I think it is really easy to get “teched out” with regard to using too many data devices during exercise. I think it’s important for you to understand exactly what you’re looking to get out of using a HRM or GPS watch or whatever else device you have. For me, I settle for the simpler devices because they fit with what I want in my training. For you, that may mean a more elaborate device or, perhaps, no devices. It’s all up to you.







